Toll FREE: 1.877.965.2140
International: 1.805.322.0005


Lipocanna™
As low as $42.95 per bottle


Medical Cannabis (Medical Marijuana and Hemp)
Medical marijuana has a long history of medicinal use in many cultures, dating back thousands of years.
Ever since five-year old Charlotte Fig was featured on the 2013 CNN documentary "Weed" . . .
interest in CBD and medical marijuana has exploded.
- Charlotte has Dravet syndrome
- She was suffering thousands of seizures per day.
- She tried many pharmaceutical drugs, but none worked.
- She experienced a remarkable improvement in her seizures after switching to a CBD-enriched extract
- "Charlotte's Web" is a cannabis strain named after Charlotte, which is low in THC and high in CBD.
With a preponderance of very promising published studies, many doctors are now recommending medical cannabis to their patients who suffer from:
- pain
- nausea
- low appetite
- anxiety
- Post-Traumatic Stress Disorder (PTSD)
- sleep problems
- muscle spasms
- multiple sclerosis
- epilepsy (seizure disorders)
- autism
Medical cannabis exists in several forms:
- flowers (aka buds), which are harvested naturally from the female cannabis plant
- can come from: marijuana (high resin plants) or hemp (low resin plants)
- can be either of 2 species: Cannabis Sativa or Cannabis Indica.
- can be any strain (out of hundreds) each with unique profiles and effects.
- extracted products, which are processed or derived from cannabis buds in a lab
- concentrates
- tinctures ar infused oils
- liposomes or Micelles
- capsules and ediibles
- pharmaceutical drugs, which are synthesized in a lab
- Dronabinol
- Nabilone
- Epidiolex
Hemp, which has been used industrially for centuries has become very popular recently due to the legal issues associated with medical marijuana products.
Because hemp is a low resin plant, hemp buds contain no more than 3.5% CBD (and less than .3% THC), so they offer very little health benefits when smoked or vaped in their unprocessed form. However, extracted hemp concentrates are chemically identical to marijuana extracts (of equal concentration) (made from low THC plants) and can be quite effectively vaped and/or taken orally. Hemp extract infused in oil (not to be confused with hemp seed oil, which is primarily used in cooking) is the most popular health supporting hemp product.
Cannabis contains a rich profile of cannabinoids (113 identified so far) that interact with our bodies in unique and sophisticated ways via the human endocannabinoid system. Cannabis also contains some non-cannabinoid substances.
The main compounds found in cannabis are:
- ∆9-tetrahydrocannabinol (THC)
- Cannabidiol (CBD)
- Cannabinol (CBN)
- Terpenoids
Chances are you've heard about THC and CBD, as they are the most well known cannabinoids (also the most prevalent compounds) whose precursors are found in the cannabis plant.
The average person probably knows that THC gets you high and CBD doesn't, but there's actually far more to these cannabinoids than this over simplification would suggest.
While cannabinoids have gotten much of the glory over the years, terpenoids are now the rising stars amongst cannabis researchers and cannabis consumers as well.
Medical marijuana can be administrated by:
- smoking
- vaping
- eating cannabis edibles
- oral consumption of capsules, pills, lozenges, tinctures or sprays
- sublingual drops
- topical sprays, creams or ointments
- dermal patches
Medical hemp products consist primarily of extracts infused in oil for oral use and pure extracts for vaping.
Legal Status
Aside from the tremendous health supporting properties of cannabis, hemp is also a great source of plant fiber with a long history in the textile industrial as well. However, for political reasons, hemp has been unfairly vilified.
- Beginning in the early 1900's, most states restricted cannabis use, requiring it to be labeled as a poison.
- By the 1920's hemp was outright prohibited.
- By the "Reefer Madness" days of the mid 1930's, every state regulated hemp as a drug. Cannabis was officially outlawed for ANY use with the passage of the Controlled Substances Act (CSA) of 1970.
- Many states and jurisdictions have continued to implement policies that conflict with federal law, beginning with the passage of California's Proposition 215 in 1996.
- In 2012 the first states legalized recreational use of marijuana.
- In 2014 the Rohrabacher-Farr amendment was enacted, limiting the ability of federal law to be enforced in states where medical cannabis has been legalized.
- by 2016, a majority of states had legalized medical cannabis.
- in 2018 President Trump signed into law "the farm law", which deregulates industrial hemp (not marijuana), essentially releasing hemp from the "chains" of the CSA.
- Accordingly, the DEA (drug enforcement administration) is now out of the picture, but The FDA (food and drug administration) is not. . .
- The FDA has taken the position that CBD can not be labeled as a dietary supplement, because it was not in commerce prior to 1994 (the year the Dietary Supplement Health and Education Act, DSHEA, was enacted), so it can not be "grandfathered in" as a dietary supplement.
- GW pharmaceuticals now has a patent on CBD and it is classified as a schedule 2 drug.
- Hemp oil has been in commerce prior to 1994, so it can be claimed on a dietary supplement label.
- According to "the farm law", which is federal and trumps state laws (no pun intended), hemp products CAN be transported across state lines, while marijuana products can NOT (even if marijuana is legal in both the state it is being transported from and the state it is being transported to).
- The irony is that even though there is no chemical difference between a THC free marijuana product and a THC free hemp product, the hemp product can be transported across state lines, while the the marijuana product can NOT.
- For this reason in order to be compliant with federal laws, medical cannabis products being sold on the internet must be limited to hemp products.
- As of 2019, 33 states and the District of Columbia have legalized cannabis for medical use. Other countries that allow the medical use of whole-plant cannabis include Australia, Canada, Chile, Colombia, Germany, Greece, Israel, Italy, the Netherlands, Peru, Poland, Portugal, and Uruguay.
Cannabinoids
Cannabinoids are a class of diverse chemical compounds that act on cannabinoid receptors in the body. They can come from cannabis plants (phytocannabinoids) or can be produced by the body (endocannabinoids). There are more than 120 identified cannabinoids found in cannabis, the best known being: THC, CBD, CBN and CBG.
THC
∆9-tetrahydrocannabinol (THC) is the main intoxicating constituent in cannabis. The intoxicating properties of THC were first described in the 1940s, however our understanding of THC dramatically improved once the Israeli scientist Rafael Mechoulam synthesized this molecule in 1965.
THC is an agonist, or activator, of the cannabinoid 1 (CB1) receptor. When cannabis is given to people who have had their CB1 receptors blocked (by a different drug, called an antagonist), cannabis cannot get them high. So, we know that the CB1 receptor must be the critical target in the brain that produces intoxication.
Brain imaging studies have shown increased blood flow to the prefrontal cortex region of the brain during THC intoxication. This region of the brain is responsible for decision-making, attention, and other executive functions, like motor skills. In short, THC intoxication can affect any of these functions to varying degrees depending on the person.
Another important factor in cannabis intoxication involves the activation of the brain's reward circuitry, which feeds our emotional and memory processes. Ultimately, the activity in these regions produces pleasurable sensations and emotions that encourage us to revisit that greasy burger place for a calorie-dense meal or ask a potential mate out on another date.
Cannabis activates the brain's reward pathway, which makes us feel good, and increases our likelihood of partaking again in the future. THC binding to CB1 receptors in the brain's reward system is a major factor in cannabis' ability to produce feelings of euphoria.
THC produces its "high" effect through the modulation of glutamate and GABA.
THC is 20 times more anti-inflammatory than aspirin, twice as anti-inflammatory as hydrocortisone.
The strong anti-emetic benefits of THC have also been well documented in adults and children, and migraine associated nausea and vomiting would certainly be another benefit of THC.
CBD
Cannabidiol (CBD) was discovered in 1940 and is the second most abundant cannabinoid found in the cannabis plant, accounting for up to 40% of the plant's extract.
There are several misunderstandings about CBD:
- Epilectics who take CBD for relief of their seizures certainly experience altered brain functioning.
- Those who take CBD for anxiety certainly experience mood changes.
The commonly held belief that CBD is "non-psychoactive", is a misnomer.
Psychoactive is a term applied to a chemical substance that acts primarily upon the central nervous system, altering brain function, and resulting in temporary changes in perception, mood, consciousness and behavior.
so strictly speaking CBD is psychoactive (as is coffee for that matter)
When people say CBD is "non-psychoactive", what they really mean is that CBD does not get you high (intoxicated with temporary changes in perception, mood, consciousness and behavior).
Regardless of the semantics, CBD may be more suitable for young patients, (or any patient for whom intoxifying effects may be undesirable). On the other hand, for those who can tolerate being high, full spectrum hemp oil (from THC dominant plants) may result in enhanced effectiveness.
- Its true that industrial hemp is CBD dominant, but even so, it contains very little CBD.
- industrial hemp (a low resin plant) contains:
- 3.5% CBD (by dry weight)
- less than .3% THC
- marijuana (a high resin plant) contains:
- as high as 20% CBD
- as high as 20% THC
- even worse, because hemp buds contain so little resin, lots of buds are required, which is bad
- Hemp is a bio accumulator (sucks toxins out of the soil).
- good for soil, but bad for medicine
- The best source of CBD is from CBD dominant marijuana.
- other good sources include:
- equally balanced marijuana strains
- THC dominant marijuana strains (if harvested early)
- Regardless of its source, CBD can be:
- part of a full spectrum product
- a single molecule isolate
- In fact, CBD is NOT an agonist for either CB1 or CB2 receptors.
- Rather, it functions to modulate the interaction of endocannabinoids and regulatory enzymes
- It also stimulates vanilloid pain receptors (TRPV1)
Another fallacy is that CBD comes from hemp, while THC comes from marijuana.
Contrary to what many websites incorrectly state, CBD does NOT attach to CB2 receptors:
As of 2019, clinical research on CBD includes investigation of potential effects on anxiety, cognition, movement disorders, pain and bone healing.
CBD can also act in concert with opioids to reduce pain
- opioid meds are required in smaller amounts if taken with CBD (opioid sparing)
- chemo therapy is required in smaller amounts if taken with CBD
- can also help overcoming opioid addiction
THC is not required for CBD to work, but these two cannabinoids do work together synergistically:
- in pain releif
- in activity with glioblastoma cancer cells
NSAI drugs relieve pain by upregulating the ECS with this same mechanism as CDB deploys, but . . .
- unlike CBD, NSAI drugs can have side effects: ulcers, heart attacks and strokes
The reason THC gets you "high", while CBD does not, is because unlike THC, CBD is exceedingly bad at activating the CB1 receptor. In fact, evidence suggests that it actually interferes with the activity of the CB1 receptor, especially in the presence of THC. When THC and CBD work together to affect CB1 receptor activity, users tend to feel a more mellow, nuanced subjective high and have a much lower chance of experiencing paranoia compared to the effects felt when CBD is absent. That's because THC activates the CB1 receptor, while CBD inhibits it. The presence of both cannabinoids balances the effects.
In the United States, the CBD drug Epidiolex has been approved by the FDA for treatment of two epilepsy disorders. Side effects of long-term use listed on the Epidiolex label include somnolence, decreased appetite, diarrhea, fatigue, malaise, weakness, sleeping problems, and others.
The U.S. Drug Enforcement Administration has assigned Epidiolex a Schedule V classification while non-Epidiolex CBD remains a Schedule I drug prohibited for any use. CBD is not scheduled under any United Nations drug control treaties, and in 2018 the World Health Organization recommended that it remain unscheduled.
CBN
Cannabinol (CBN) was the first cannabinoid to be identified by scientists, but is considered a "minor cannabinoid".
As THC oxidizes (i.e. exposure to oxygen over time), it converts to CBN. This is why aged, poorly stored cannabis is likely to have higher levels of CBN than fresh flower in an air-tight container.
CBN can make users sleepy.
CBN has been prescribed for:
- Pain relief
- Anti-insomnia
- Promotes growth of bone cells
- Antibacterial
- Anti-inflammatory
- Anti-convulsive
- Appetite stimulant
CBG
Cannabigerol (CBG) is is a minor constituent of cannabis (somewhere below 1%), and is thus considered a "minor cannabinoid".
In vitro studies indicate CBG has high affinity as an α2-adrenergic receptor agonist, moderate affinity as a 5-HT1A receptor antagonist, and low affinity as a CB1 receptor antagonist. Other in vitro research shows it has low-affinity binding at CB2 receptors.
Terpenes and Terpenoids
Terpenes are the organic molecules in cannabis plants, which are responsible for its aroma and flavor. More than 200 terpenes have been discovered in the cannabis plant so far. Each cannabis plant variety has a unique aroma and taste, because it has a unique profile of terpenes, The proportional makeup of terpenes in cannabis is directly impacted by both the spectrum and intensity of its light exposure while growing.
Terpenes do more than provide flavor and aroma. They also support other cannabis molecules in producing desired effects. We call this the "entourage effect" (aka "ensemble effect"), and it's the reason terpenes have become such a critical area of cannabis research. The "entourage effect" suggests that the right cocktail of cannabis compounds will prove more potent and effective than an isolated compound.
There is a lot of confusion about the terms "terpene" and "terpenoid", which are often incorrectly used interchangeably. Terpenes are found in cannabis plants. When cannabis buds are dried and cured, the terpenes oxidize and become terpenoids. In other words . . . cannabis plants contain terpenes, while dried and cured cannabis buds contain terpenoids.
Terpenoids and cannabinoids may either exaggerate or suppress one another's effects, depending on which combination is present and how an individual responds to it. Mounting scientific evidence suggests that terpenoids also play a considerable role in not only tempering the intoxicating effects of THC, but also creating synergy with phytocannabinoids and even increasing their therapeutic value.
Cannabis terpenoids are thought to increase the uptake of cannabinoids in the intestines, enhance receptor binding mechanisms and transmembrane interaction, and impact metabolism too
Terpenes are formed in trichomes, which are the sticky glandular hairs found primarily in the cannabis buds. The trichomes have a crystal-like sheen and sticky feel because they contain resin glands that produce terpenes and cannabinoid acids such as THCA and CBDA, which turn into THC and CBD when decarboxylated. Essentially all of the desirable compounds in cannabis are found in the trichomes.
Terpenes are not unique to cannabis. Other plants also contain terpenes. Being the primary components of essential oils (created by plants), terpenes help protect the plant against herbivores, insects, and other environmental dangers. They're also responsible for a plant's regeneration, oxygenation and immunity defense, which is why cannabis researchers are investigating if terpenes may serve as immunity boosters in humans.
Chemically, there really is no difference between specific terpenes extracted from different plants. When it comes to function, what's more important than the specific terpene, is the other specific compounds present along with the terpene. In the case of cannabinoids, which are uniquely found in cannabis, terpenes interact with and influence the effects of cannabinoids.
Terpene preservation has never been more important to the cannabis market than it is now. Growing, harvest, and curing conditions all have an effect on terpene expression, and they can all contribute to the terpene-heavy cultivars that today's cannabis consumers are looking for.
In order to get a rich terpene profile, cannabis plants should neither be harvested too early nor too late. Harvesting too early may cut trichomes off from full cannabinoid and terpene production, while harvesting too late may produce trichomes that have decreased in chemical potency, or broken off entirely. Properly ripe trichomes will be bold, distinct, and translucent on the plant's surface, and they'll be rich in terpenes. Cannabis emitting a strong pungent fragrance is commonly referred to as being "skunky", which is very desirable and considered an indicator of high quality.
Other factors that influence terpene production include growing at sufficiently cool temperatures (77-80℉, or 25-26.67℃, during the day and roughly 7-10 degrees colder at night) and drying under sufficiently cool temperatures (between 65-75℉, or 18.33-24℃) to reduce terpene evaporation. Lastly, being as gentle as possible with cannabis flower in every step of the cultivation process will increase a grower's chances of coming up with a terpenoid-rich final product.
A huge factor in the cannabis industry's current terpene boom is the growing popularity of "dabbing" (the act of inhaling vaporized cannabis concentrates through a temperature-specific heating method such as a dab rig, e-rig or vaporizer). Dabbing concentrates at high temperatures typically results in a smooth, tasty cannabis vapor-rich in terpene flavors. What many dabbers may not be aware of is the possibility that terpenes produce toxic chemicals when super-heated. According to a study from Portland State University, vaporizing terpenoids at the high temperatures required for dabbing may produce the toxicants methacrolein and benzene, which have been linked to certain cancers. So, if you want to enjoy a flavorful dab without heating the terpenoids to toxicity, dab at as low a temperature as possible.
Although hundreds of different terpenes have been found in cannabis, only a select group of them are sufficiently present. These are the 11 most prominent terpenes in cannabis, along with their aromas, boiling points, and potential health benefits as shown in experiments on animals.
- Myrcene and Caryophyllene
- the two most prominent terpenes in cannabis. (most cultivars are dominant in one or both.)
- Myrcene (a monoterpene) carries the signature "earthy" aroma found in most cannabis plants.
- has a boiling point of 332.6℉ (167℃)
- an effective anti-inflammatory
- may also alleviate pain
- Myrcene accounts for the sedative effect (falsely attributed to "indica") and contributes to the "couch lock" (tired effect)
- Caryophyllene carries an "herbal" aroma.
- has a boiling point of 266℉ (130℃)
- also found in hops, cloves, and rosemary
- Like myrcene, caryophyllene has both anti-inflammatory and pain relieving properties.
- Pinene
- Pinene is one of the most commonly expressed terpenes in nature.
- responsible for the" piney" aroma of certain cannabis cultivars
- found in pine trees and other conifers
- has anti-inflammatory properties
- may help to protect from ulcers
- may help improve airflow to the lungs
- has a boiling point of 311℉ (155℃)
- Limonene
- In addition to being found in cannabis, limonene is commonly found in citrus fruits.
- provides the classic citrus smell
- has a boiling point of 348.8℉ (176℃)
- Limonene is commonly used in a wide variety of products, from cleaning supplies to fragrances.
- may boost immune system function
- may alleviate heartburn symptoms
- can be used as a solvent to dissolve gallstones rich in cholesterol
- uplifting on mood
- can effectively reduce or eliminate the classic THC-induced short-term memory impairment
- Terpinolene
- Terpinolene has a fresh herbal-citrus aroma.
- has a boiling point of 361.4-365℉ (183-185℃)
- commonly found in plants known for pleasant fragrances (i.e. rosemary, conifers, lilacs, apples)
- Human studies have identified terpinolene as a potential antioxidant, and animal studies have found it to have sedative properties.
- Terpinolene might eventually be used to decrease cell proliferation associated with cancer.
- Humulene
- Humulene is common cannabis terpene that's also predominant in hops.
- also present in sage, clove, basil, black pepper, and ginseng
- carries the signature "hoppy" aroma
- may be an effective topical anti-inflammatory and pain reliever
- has a boiling point of 222.8℉ (106℃)
- Linalool
- Linalool is a terpene found in rosewood, bergamot, coriander, rose, jasmine and lavender.
- has a boiling point of 388.4℉ (198℃)
- carries a very pleasant floral aroma, and is often used in soaps and perfumes.
- In addition to potentially reducing inflammation and inflammatory pain like several other terpenes, linalool has several unique potential health benefits.
- inhibits the growth of fungal infections outside the human body, particularly as they arise from the yeast infection candida.
- It also has anticonvulsant and sedative properties.
- Ocimene
- Ocimene has a strong, sweet, herbal scent.
- has a boiling point of 212℉ (100℃)
- found in a wide variety of plant life, including mint, mangoes, basil, and orchids
- Omicene can act as an anti-inflammatory, and may have antiviral and antifungal properties.
- Nerolidol
- Nerolidol is characterized by a singularly woody aroma
- used in a wide variety of cosmetic and cleaning products has been studied for its potential as an antifungal, antioxidant, anti-microbial, and anti-inflammatory agent.
- Nerolidol may even help other drugs penetrate the skin for more effective topical delivery.
- has a boiling point of 251.6℉ (122℃)
- Bisabolol
- Bisabolol has a mild floral scent, and is frequently used in fragrances and cosmetics.
- has a boiling point of 307.4℉ (153℃)
- Bisabolol has long been thought to heal the skin.
- Animal studies have confirmed that bisabolol may specifically reduce skin inflammation.
- Guaiol
- Guaiol is found in guaiacum and cypress pine.
- has a quintessentially piney aroma
- has a boiling point of 197.6℉ (92℃).
- has been identified as a potential antimicrobial, as well as an inhibitor of lung cancer cell growth.
- Guaiol is also a central component of essential oils in Xylopia sericea fruits that have potential antibacterial and antioxidant properties.
Cannabis Chemotypes
Most people know cannabis plants can be either of 2 species (cannabis sativa or cannabis indica),
but much of what most people think they know about the sativa and indica species is actually wrong.
Sure, the description of how the morphology between the species differ is generally accurate . . .
- sativa plants are characterised as:
- tall and lanky with narrow leaves
- indica plants are characterised as:
- short and bushy with broad leaves
but, the long held and persistent belief that species is the most important factor in determining the kind of effect a cannabis user is likely to experience. is a misnomer, being way too much of a generality to reliably predict effect.
According to what I call the "species-folklore fallacy":
- the effect of sativa is characterised as
- uplifting, energetic, creative, euphoric, spacey, cerebrally-focused, and better for day use
- the effect of indica is characterised as
- calming, relaxing, sedative, full body - "body buzz", and better for night use
There are several reasons why this "species-folklore fallacy" exists and persists:
- The Indica/Sativa taxonomy was originally adapted to describe a cannabis plant's physical traits (morphology) and geographic origin (landrace), NOT its chemical makeup (chemotype).
- This very much outdated convention was established long before:
- we knew anything about cannabis terpenoids and the interaction they have with cannabinoids.
- aggressive hybrid breeding vastly diversified cannabis chemotypes
- Marketers in the cannabis industry perpetuate the "folklore out of ignorance and/or sales hype.
Research suggests these effects are not likely due purely to CBD:THC ratios, as there are no significant differences in CBD:THC ratios between Sativa and Indica strains. Rather these different subjective effects are likely due to varying ratios of major cannabinoids as well as minor cannabinoids, terpenes and probably additional phytochemicals
Understandably, many cannabis cunsumers are confused, but here's the bottom line:
- When it comes to predicting cannabis effects . . . the chemotype is far more important than the species.
- what ratio of cannabinoids are present
- which terpenes are present (and in what proportion)
Different strains do have different chemotypes and can be classified by their cannabinoid dominance:
- THC-dominant strains
- primarily chosen by those seeking a potent euphoric experience.
- chosen by those with: pain, depression, anxiety, insomnia, and more.
- best for cancer, neurological disease, gut issues
- better for glioblastoma cancer patients
- Example:
- Bedrocan® (THC:CBD ratio of 22:1)
- CBD-dominant strains
- used by those highly sensitive to THC or patients needing clear-headed symptom relief
- best for anxiety, spastics, seizures
- preferred by neuroblastoma cancer patients
- Examples:
- ACDC, Ringo's gift, Valentine X, Remedy, Harlequin, Cannatonic, Sour Tsunami(THC:CBD ratio of of 1:10)
- Balanced THC/CBD strains
- provides mild euphoria alongside symptom relief.
- good choice for novice consumers seeking an introduction to cannabis' signature high.
- Example
- Jamaican Lion, Omrita RX, Blue Jay Way (THC:CBD ratio of 1:1, or 3:2)
Its worth noting that cannabis buds can be THC rich or CBD rich
- This has nothing to do with the plant's strain
- Rather it has to do with when the buds are harvested
- CBD matures before THC.
- An early harvest will favor a CBD rich product (even if the strain is THC dominant)
Its also worth noting that medical cannabis can come from marijuana or hemp plants.
- Many people incorrectly think THC comes from marijuana, while CBD comes from hemp.
- The actual difference is that marijuana is a high resin plant, while hemp is a low resin plant.
- marijuana plants:
- contain as high as 20% CBD or THC
- extracts do not need thinning agents, viable "as is"
- industrial hemp plants
- contains less than .3% THC
- contain 3.5% CBD (by dry weight)
As important as cannabinoid profile is in predicting effect . . .
the importance of the terpenoid profile can not be understated.
- strains which were considered "mostly indica" were characterized by dominancy of β-myrcene, present in high relative contents, with limonene or α-pinene as second most abundant terpenoid,
- while strains that were said to be "mostly sativa" were characterized by more complex terpene profiles, with some strains having α-terpinolene or α-pinene as dominant terpenoid, and some strains having β-myrcene as dominant terpenoid with α-terpinolene or trans-β-ocimene as second most abundant terpenoid.
- Breeding for specific terpenoids in plants is a fascinating research topic.
- Terpenoids analysis, combined with cannabinoids and flavonoids analyses, are essential for the metabolic fingerprinting of pharmaceutical cultivars, which could lead to the selection of chemotypes for specific medical effects.
A recent study
Variations in terpene profiles of different strains of Cannabis sativa
L. Acta Horticulturae 925:115-121
demonstrated that:
Full Spectrum versus single molecule Isolates
Medical marijuana is a botanical (a medicinal preparation obtained from a plant) . . . a whole plant (full spectrum) product, which does not rely on any one of its compounds to produce its benefit
- Being a full spectrum botanical, the FDA deems cannabis a dietary supplement.
- Single molecule cannabis isolates, on the other hand, are deemed by the FDA as drugs.
There are certainly plenty of good applications for single molecule isolates:
- Single molecule CBD has anti tumor, anti spasmodic, anti convulsive, anti depressive, anti psychotic, anti addictive anti anxiety, anti biotic and analgesic properties
- Terpenoids can have a medicinal effect of their own as an anti-inflammatory, antibiotic or analgesic.
- the terpene myrcene is good for pain, but also makes you tired.
- the terpene Caryophyllene is also good for pain, although it works through a totally different mechanism than myrcene does (interacting with CB2 receptors).
Full spectrum cannabis however, is generally considered to be safer and more effective in supporting homeostasis than any single molecule cannabis isolate.
- Cannabis contains over 100 cannabinoids plus terpenoids, which all nourish and support the ECS.
- The "Entourage Effect" is a phrase coined by Raphael Mechoulam and S. Ben-Shabat (in 1998) to describe how the "active and "inactive" components present in cannabis (cannabinoids, terpenoids, flavonoids and cannabidiolic acids) work together in concert to create the clinical cannabis effects.
-
THC causes intoxication by activating the CB1 receptors, however If CBD is also present . . .
THC will also stimulate CB2 receptors (involved in pain and immune response) - Because CBD reduces the intoxicating effects of THC, larger doses of THC can be administered (when CBD is also present) and thus greater benefits can be achieved [Pertwee, 2000; Russo and Guy, 2006].
- A recent study on children with high-level epilepsy, compared the response of single molecule isolates and full spectrum plant extracts
- regardless of which treatment they received, 31% of all subjects responded favorably.
- Those with favorable responses in the "single molecule isolate group", experienced a 50% reduction in seizures.
- Those with favorable responses in the "full spectrum extract group", experienced a 71% reduction in seizures.
- CBD and THC are synergists . . . CBD is generally more effective when combined with THC.
- CBD improves THC efficacy for relief of neuropathic pain and autoimmune diseases.
- THC and CBD each have anti tumor effects, but CBD magnifies THC effect on brain cancer
- THCA also has a synergistic effect on CBD
Pharmaceuticals
Botanicals are considered whole plant nutraceuticals (which are dietary supplements) and can NOT be patented.
Single molecule isolates and synthetic cannabinoids are both considered pharmaceuticals and CAN be patented.
Although there has not been a lot of research comparing the effects of botanicals to single molecule isolates or synthetic cannabinoids, evidence suggests that the botanicals may be safer and just as effective (if not more so) than their pharmaceutical counterparts.
- Botanicals contains over 525 known phytonutrients, which contribute to an "entourage effect" that cannot be achieved by any single molecule isolate or synthetic cannabinoid.
- Many patients, who have tried both botanical and pharmaceutical forms, prefer the botanicals.
- 45% of patients, who were prescribed Marinol, reported negative side effects, and stopped using the drug after completing only one round of the prescription.
Big Pharma, does all it can to suppress any research that might show botanicals to be safer and/or more effective than the drugs they push.
- Lobbyists like Insys, work to prevent the downgrade of botanical marijuana from a Schedule I substance.
- Remaining a Schedule I drug at the federal level, stifles research because approval is then required from 4 federal agencies before any studies can be conducted. An even then, only with "research-grade" marijuana, which does not necessarily have the same effects as other available strains.
- The resulting lack of concrete medical evidence on botanical marijuana's benefits makes it easier for Big Pharma to argue that their drugs are better and safer for patients, despite plausible theories to the contrary.
- With their significant resources and virtual monopoly on accepted research, Big Pharma will continue to downplay the potential benefits of botanicals and mislead the public about the superiority of their drugs.
Botanical marijuana is significantly cheaper than pharmaceuticals drugs.
- Marinol sells for $18 per 5 mg capsule, the equivalent of $3,600 per gram.
- Botanical marijuana can be obtained for $15 a gram
The most common pharmaceutical medical marijuana drugs include:
Epidiolex
-
an FDA approved drug for for seizures associated with:
- Lennox-Gastaut syndrome
- Dravet Syndrome
- the first CBD (single molecule isolate) drug approved by the FDA (in June 2018).
- GW Pharmaceuticals holds the patent for Epidiolex
- requires a large dose that must be determined precisely (on an individual basis) to be effective
- formulated as a liquid to be administered oral mucosally, using a syringe
- Side effects include:
- sleepiness
- decreased appetite
- diarrhea
- increase in liver enzymes
- feeling very tired and weak
- rash
- sleep problems
- infections
Nabiximols (Sativex):
- for the treatment of spasticity, neuropathic pain, and other symptoms of multiple sclerosis
- GW Pharmaceuticals holds the patent for Sativex
- a balanced oil (1:1 ratio of CBD:THC ) derived from botanical marijuana
- under-the-tongue spray (tincture)
- may be most effective pharmaceutical cannabis based drug for pain
- Side effects include:
- abdominal (stomach) pain
- appetite changes (increase or decrease)
- balance problems
- burning sensation in the mouth
- constipation
- cough
- diarrhea
- dizziness
- drowsiness
- dry mouth
- forgetfulness or poor concentration
- mood changes
- nausea
- panic attacks
- sore throat
- soreness or stinging sensation in mouth
- spinning sensation
- tiredness
- trouble sleeping
- trouble urinating
- unusual taste in the mouth
- weakness
Dronabinol (Marinol and Syndros):
- synthetic THC
- approved by the FDA, as safe and effective for:
- HIV/AIDS induced anorexia
- chemotherapy induced nausea and vomiting
- appetite stimulant, antiemetic, and sleep apnea reliever
- Solvay Pharmaceuticals holds the patent for Dronabinol
- formulated as an oily resin in capsules
- most users who have reported that the effect is not at all fun (like marijuana).
- not likely to penetrate the recreational market
- Side effects include:
- drowsiness
- cotton-mouth
- euphoria
- tachycardia
- postural hypotension
- lethargy
- slurred speech
- decreased motor coordination
Nabilone (Cesamet):
- another synthetic THC
- a cannabinoid agonist with superior bioavailability to dronabinol
- has a more predictable dose-response relationship
- has less individual variability in drug response
- used as a treatment for nausea and vomiting associated with cancer chemotherapy
- formulated as a capsule for oral administration
- Side effects include:
- dizziness
- drowsiness
- euphoria "high"
- ataxia
- anxiety
- disorientation
- depression
- hallucinations
- psychosis
- tachycardia
- orthostatic hypertension
Cannabis Dosage
The therapeutic dosage of medical cannabis varies from person to person and depends on several factors:
- the type and severity of the medical condition
- the level of cannabis experience the patient has
- the delivery method used
There is no standard "one size fits all"
Dosage ranges from:
- 1mg/kg (min dosage)
- 5mg/kg (average dose)
- 20mg/kg (upper range of dosage)
- even up to 100mg/kg doses for seizures
Equivalency:
- 1 gram of dried cannabis = 77 mL of full spectrum oil
Health Canada has created the "Equivalency Factor":
- 1 gram of dried cannabis = 125 mg of THC oil
- 1 mL of oil = 25 mg of THC
- Has limited usefulness, as it fails to consider differences between THC-rich, CBD-rich and balanced blends
According to Martin A. Lee (co-founder and director of Project CBD)
Optimizing one's therapeutic use of cannabis may entail some experimentation. In essence, the goal is to administer consistent, measurable doses of a CBD-rich cannabis remedy with as much THC as a person is comfortable with.
A good rule of thumb is: Start low and go slow.
- When smoking or using a vaporizer, patients should wait a few minutes between inhalations to let the dose be fully realized in order to gauge the strength of the effect.
- The average dose of medical marijuana is 1 to 3 g/day when smoked or vaporized.
- In one recent Canadian study, 25 mg of pharmaceutical-grade cannabis with a THC content of 9.4% was effective in reducing intensity of pain, improved sleep and was well tolerated when smoked as a single inhalation 3x/day for five days.
- With edible oils, patients should exercise caution when dosing for the first time.
- allowing at least an hour for the product to work through the digestive track and take effect,
- then waiting at least four hours before taking a second dose.
- High doses of CBD are not always more effective than lower doses.
- A CBD dose of as little as 2.5 mg combined with a small amount of THC can have a therapeutic effect.
- Full-spectrum CBD-rich cannabis oil (with a small amount of THC) is efficacious at much lower doses and has a much wider therapeutic window than pure, pharmaceutical-grade CBD.
- Cancer patients who received 21 mg/day of Sativex experienced significant reductions in pain,
- more so than cancer patients who received 52 mg of Sativex,
- while those who were given 83 mg of Sativex reduced their pain no better than a placebo.
- In clinical trials of epidiolex, children with catastrophic seizure disorders were given up to 50 mg of epidiolex per kg of body weight. Such high doses caused interactions with other anticonvulsant medications, requiring adjustments of the latter to avoid a toxic overdose.
- Dr. Bonni Goldstein (author of Cannabis Revealed), typically starts with a much lower dose of full spectrum CBD-rich oil (1 mg CBD/kg of body weight) for epileptic children - with the understanding that the dose may have to be lowered or raised depending on the initial response. If necessary, Goldstein increases the dose of CBD by increments of 0.5 mg/kg until a threshold of 5 mg/kg of body weight is reached. And that amount may also need to be adjusted.
- Kids, adults and animals metabolize drugs differently.
- It may seem counterintuitive, but young children can actually tolerate higher doses of cannabis oil concentrates, (including THC-rich formulations) than adults can. Thus, it's not a good idea to calculate dosage for an adult based on what works for a child.
- If 1 mg/kg of CBD is an appropriate starting dose for a child, and an adult weighs 15 times more than the child, one should not assume that the correct CBD starting dose for the grown-up is 15mg/kg of body weight. That could be way too high a dose. While CBD has no known adverse effects at any dose, an excessive amount of CBD may be less effective than a moderate dose.
- Similarly, it's not a good idea to devise a dosage regimen based on data from animal studies, which usually involve high doses of single-molecule cannabinoids. Human metabolism differs from mice and rats, and data from animal models doesn't always translate to human experience.
- When ingesting THC-rich cannabis products (with little CBD), microdosing as little as 2.5 mg THC can provide symptom relief without making a person feel high.
- If well tolerated, the amount of THC can be increased to 15 mg (divided equally throughout the day).
- Doses exceeding 20-30 mg/day (or a single dose of 10 mg or more) may cause unwanted side effects.
- A balanced ratio of CBD and THC could have a greater therapeutic impact than either CBD or THC alone. so its good to adjust the amount of CBD and THC until you find the sweet spot.
- When using the full-spectrum hemp oil for insomnia, the 25-milligram range seems to be most effective.
- Medical marijuana does not need to be taken per some schedule, can be taken when needed:
- daily
- multiple times per day
- every other hour (not uncommon and not considered addiction)
- should be taken at least an hour or two before bedtime
When we look at the research on dosing, unfortunately, we must rely mostly on studies conducted by GW Pharmaceuticals, which were done with isolated, purified CBD.
- An alternative 2015 study, out of Israel, showed that a study group using full-spectrum oils had superior outcomes compared to the group taking the single molecule isolates.
- While the bulk of the dosing studies were conducted using doses in the couple of hundred milligram range, many clinicians who are using much smaller does- anywhere from 10 to 25 milligrams a day are reporting quite remarkably responses.
Cannabis Contraindications
In 2018 the World Health Organization (WHO) re-rated the risk of using cannabis:
Cannabis is a "relatively safe drug" that has never led to overdose-related deaths. Acute side effects primarily affect the mind and psychomotoric functions as well as the heart and circulatory system. These effects usually vanish after a short period of time.
Due to its psychotropic effects cannabis medication is contraindicated for patients suffering from severe personality disorders and who have a higher risk for psychoses.
The active substances of cannabis, THC and CBD, are metabolized - like many other pharmaceutical substances - via the hepatic cytochrome P450 system (CYP450), which may result in interferences with other drugs.
The abuse risk of cannabis is very low compared to other substances. Nevertheless, the long-term, heavy use of cannabis, especially during adolescence, can lead to psychological and behavioral disorders and should therefore be therapeutically clarified and monitored.
In 2014, the College of Family Physicians of Canada (CFPC) produced its first guideline for physicians, focusing on cannabis for the treatment of chronic pain or anxiety. In their document, the CPFC not only listed what sort of people might be inappropriate candidates for medical cannabis, but also rated the level of the research evidence for their recommendations. Their rating scheme consisted of three levels:
- Level I - evidence is the strongest (well-conducted controlled trials or meta-analyses),
- Level II - evidence is 2nd strongest (well-conducted observational studies),
- Level III- weakest evidence (consensus of the expert members of the committee writing the guidelines).
To summarize, in this document the CFPC advised doctors to not authorize medical cannabis to patients who:
- Are under the age of 25 (Level II)
- Have a personal history or strong family history of psychosis (Level II)
- Have a current or past cannabis use disorder or another active substance use disorder (Level III)
- Have cardiovascular or respiratory disease (Level III)
- Are pregnant, planning to become pregnant or are breastfeeding (Level II)
In addition, it said caution should be used in recommending cannabis for patients who:
- Have a mood or anxiety disorder (Level II)
- Smoke tobacco (Level II)
- Have risk factors for cardiovascular disease (heart disease and stroke) (Level III)
- Are heavy users of alcohol or take high doses of opioids, benzodiazepines (a class of tranquilizers) or other prescription or over-the-counter sedatives (Level III)
In 2013, the Canadian College of Physicians and Surgeons of Canada asked the federal government to develop explicit indications, precautions and contraindications for medical cannabis, so doctors could evaluate which of their patients should, or should not, be given access to medical cannabis.
Although they disclaimed any conclusions about the appropriate use of cannabis (marihuana) or cannabinoids for medical purposes, they did state that based on contraindications for existing synthetic cannabis medications (nabilone and dronabinol) and the cannabis extract dronabinol, Health Canada suggested the risk/benefit ratio of cannabis needs to be carefully and individually considered for people who:
- Are under the age or 18
- Have a history of hypersensitivity to any cannabinoid or to smoke (if the cannabis is smoked)
- Have severe cardio-pulmonary disease with occasional hypotension (low blood pressure), possible hypertension (high blood pressure), syncope (loss of consciousness) or tachycardia (rapid heart rate)
- Have respiratory diseases such as asthma or chronic obstructive pulmonary disease (COPD)
- Patients with severe liver or renal disease, including chronic hepatitis C
- Have a personal history of psychiatric disorders or a family history of schizophrenia
- Have a history of substance abuse
- Are women of childbearing age not on a reliable contraceptive, planning to become pregnancy, are pregnant, or are breastfeeding.
- In additional, it suggests medical cannabis should be used with caution in people who have mood disorders or are taking sedatives or other psychoactive drugs.
According to Dr. Ethan Russo, medical marijuana can adversely interact with other drugs (slows their metabolism resulting in much longer half lives)
- CBD inhibits the cytochrome P450 enzyme, which is involved in metabolizing many drugs. Compounds in grapefruit inhibit the same enzyme group, which is why physicians advice patients not to eat grapefruit shortly before or after taking a medication. By inhibiting cytochrome P450, CBD can either reduce or increase the effects of other drugs. In some situations, it may be advisable for a physician to monitor a patient's blood levels of other medications while taking CBD.
- In extreme doses when used in isolation, CBD can induce sedation in combination with other drugs (for example clobazone, used to treat seizure disorders)
Cannabis Side Effects
Many substances that have beneficial effects also have unwanted side effects. Cannabis is no exception.
THC rich products, such as buds, extracts and pharmaceutical CB1 agonists (i.e. Dronabinol, Nabilon) can exhibit a range of short term side effects, which are mainly mediated by CB1 receptor activation.
THC side effects primarily impact:
- the mind and psychomotoric function
- the heart and circulation (tachycardia, vasodilation, drop in blood pressure, dizziness, syncope).
Psychoactive effects are common and are usually perceived as pleasant and relaxing and can therefore be used therapeutically. However, for some, these effects can manifest as:
- dysphoria
- anxiety
- confusion
- panic
- paranoia
These side effects are generally associated with the dose being too high.
- CBD can counter these effects.
Other known side effects include:
- dryness of the mouth
- increased appetite
- decreased formation of tears and reddened inflamed eyes
- altered perception of time and senses
- disruptions in orientation and balance
- muscle weakness
- restlessness
- insomnia
- rapid pulse
- dizziness
- headache
- hot or cold hands and feet
- short term memory loss
CBD is well tolerated, even in large doses. Research suggests any side effects that do occur with CBD use are likely the result of drug-to-drug interactions between CBD and other medications.
Cannabis Delivery Systems
Medical Marijuana (like any medication) needs to enter the blood system, before it can reach its target sites and cause its desired effects.
- Bioavailability can be defined as the degree to which a medication can be measured in the blood stream.
- Many factors impact bioavailability of a medication:
- its molecular size
- the extent to which it breakdown in the gastrointestinal (GI) tract
- its solubility (and thus its absorption) in the small intestine
- the degree to which "first pass metabolism" breaks it down in liver
- the gut health of the subject
- The delivery system (the way a substance gets to its target site) is a big factor in:
- Bioavailability
- How intense the effects are
- How long it takes for onset of effects
- How long the effects last
Delivery systems available for medical cannabis include:
inhalation (smoking or vaping), oral (sublingual or swallowed), topical and rectal suppositories.
- Intravenous (IV):
- 100% bioavailable, but not practical
- VERY few people (if any) utilize this delivery system.
- Inhalation (smoking or vaping):
- 34-46% bioavailable
- bypasses the (GI) tract and "first pass metabolism", which accounts for it high bioavailability
- The bioavailability of THC inhalation is reported to be as high as 56%.
- very little difference (if any) between bioavailability of vaping compared to smoking
-
Difficult to accurately measure because of smoking/vaping variables -
size and spacing of puffs, hold time, and volume of inhalation - Fastest acting delivery system
- when smoke or vapor enters the lungs it quickly passes directly into the bloodstream.
- Health risks
- Smoking
- Lingering second-hand smoke may be undesirable for family members.
- can cause bronchitis (does not cause emphasema, COPD or lung cancer)
- Vaping
- Only high quality, pure "vape oils" should be used (not infused oils).
- safety concerns with flavors and aromas in many vape pen cartirdges
- important temperatures pertaining to the vaping of dried buds:
- decarboxylation takes place at 240℉-250℉ (115.6℃-121.1℃)
- THC vaporizes at 315℉ (157.2℃)
- CBD vaporizes at 356℉ (180℃)
- most terpenes vaporize between 311℉ and 388℉ (155℃ and 197.8℃)
- combustion occurs at 450℉ (232.2℃)
- optimal vaporization temperature is between 320℉ and 410℉ (164.4℃ and 210℃)
- 360℉ (182.2℃) is probably best
- Oral consumption:
- Sublingual (under the tongue):
- 12-35% bioavailability (best oral delivery system)
- absorbed through the mucous membrane under the tongue. Capillaries in the connective tissue diffuse the substance, facilitating its entry into the bloodstream.
- bypasses the digestive system and liver "first pass metabolism". preserving more of the actives allowing them to enter the bloodstream faster
- can be delivered with tinctures, concentrates, lozenges, and sprays
- Swallowing:
- 4-20% bioavailability
- popular due to its ease of use
- must go through the gastrointestinal tract and then into the liver, where it suffers further breakdown ("first pass metabolism") reducing bioavailability.
- can take as long as two hours to enter the bloodstream, but has longer lasting effects
- A study (Huestis, 2009-published by the U.S. National Library of Medicine) suggests that swallowing with fatty acids may bypass the "first pass effect" and increase absorption rates.
- can be delivered with capsules, edibles, oils and tinctures
- Capsules:
- Popular amongst doctors and patients because:
- elimination of measurement mistakes with dosages
- easier and more convenient than using syringes to measure dose
- no sugar
- not cultivar or strain-specific
- Infused Oils:
- cannabis extracts that have been infused into an oil
- liquid at room temperature
- already "active" (decarboxylated)
- don't need to be heated or vaporized . . . just ingested.
- different from vape oil (shouldn't be smoked or vaped)
- will change the compounds and potency of the cannabinoids
- Tinctures (aka green or golden dragon):
- extracts dissolved in ethyl alcohol (ethanol)
- Solvent concentrations of 25-60% are common.
- 15-45 minutes onset, peak effects at about 90 minutes
- Edibles:
- 10% bioavailability
- Edible snacks are fun, but are a not very effective delivery system.
- they're a nutritional disaster containing lots of sugar and salt
- Plus, sugar and salt both act against hemp actives
- Liposomes and Micelles:
- Liposomes and Micelles are similar (but different) delivery systems that involve the encapsulation of a nutrient (the payload) with a lipid to improve its bioavailability.
- Liposomes contain a lipid bilayer (similar to the makeup of cell membranes).
- most often composed of phospholipids (especially phosphatidylcholine)
- have an aqueous core
- most suitable for a water soluble payload
-
normally a water soluble nutrient
- can enter the blood system easily
- has difficulty integrating with or passing through a cell membrane and into a cell
- theoretically, a liposome can facilitate the transport of its water soluble payload intact (through the digestive system) and then through the cell membrane of its target cell.
- Micelles contain a lipid monolayer
- improves water solubility of its payload
- theoretically delivers more payload to the blood stream, but not necessarily more to the target cell membrane or into the target cell
- The biggest drawback with both liposomes and micelles is stability.
- They have very short shelf lives and quickly degrade into emulsions.
- Manufacturers of both liposomal and mycelized medical marijuana products make many claims about how superior the bioavailability of their products are.
- They show impressive graphs, which supposedly demonstrate their superior bioavailability.
- None of these manufacturers was able to refer me to a single published clinical study to substantiate their product claims.
- I searched extensively on the pubmed website, but could not find ANY published studies to back up these claims.
- I don't know how they can even plot a graph with data that does not seem to exist.
- One product website shows a beautiful graph, but did not have any vertical "y"axis scale. When I inquired what the "y" axis scale was, I was told "its relative." Not exactly a professional response.
- Although liposomes and micelles may have some valid applications in pharmacology, I personally believe that those, who claim their liposomal and/or mycelized medical marijuana products have enhanced bioavailability, are just perpetrating a scam.
- Topical (application to the skin):
- Cannabis oils can be mixed with butters or other oils to create topicals, which can be applied to the skin.
- Topicals enter the skin and body tissues and allow for direct application and relief of affected areas for allergic skin reactions, muscle strain, inflammation, swelling, etc.
- Both THC and CBD are effective topicals, which reduce inflammation and provide pain relief.
- Topicals do not get you "high", because they do not reach the bloodstream.
- interacting with "local" cannabinoid receptors instead.
- Skin does not absorb cannabinoids very well, so its best to apply topicals very generously.
- Topical forms include: oils, creams, salves and transdermal patches
- oils:
- They do not absorb very well and are messy.
- Creams:
- cannabinoids heated into shea butter and combined with other ingredients.
- Salves (aka ointments):
- cannabinoids heated into coconut oil and combined with beeswax.
- Transdermal patches:
- The only topical CBD products able to penetrate the skin and enter the bloodstream are transdermal CBD patches. Transdermal, by its very definition, means able to cross the dermal barrier to reach the blood. The U.S. Library of Medicine discusses a study, (Hammell et al, 2016), proving the ability to CBD to be efficiently absorbed via transcutaneous methods.
- Rectal administration (suppositories):
- Many people laugh when they hear the phrase "cannabis suppository", but they are no joke.
- Suppositories are a very effective and easy to use delivery system.
- Suppositories work quickly, exerting systemic effects when they enter the rectal mucosa, spreading healing compounds quickly through nearby organs and into the bloodstream.
- Suppository users report a very diminished "high" effect.
Cannabis Extraction Methods
Extraction is a process which separates oils and waxes from botanical plant materials.
- The end product of extraction is referred to as an "extract" or "concentrate".
- Extraction can be performed either mechanically (i.e. kief etc) or through the use of solvents.
- The commercial extraction of medical marijuana is usually done with solvents.
- The most commonly used extract solvents are:
- CO2
- Hydrocarbons (butane, propane, hexane and naptha)
- Ethanol
- No one solvent is "better" than another.
- Each has its pros and cons (situation specific)
- CO2 extraction:
- To understand CO2 extraction, its important to first understand some thermodynamic concepts:
- Matter can exist in three different phases (solid, liquid and vapor).
- The boundaries that separate phase are specified by pressure (P) and temperature (T) conditions.
- The "critical point" is defined as the P and T combination (Pc and Tc) where two phases coexist.
- The "critical point" of CO2 is reached when Tc = 87.98℉ and Pc = 1,071 psi
- When CO2 reaches or exceeds its "critical point" its said to be supercritical.
- behaves as a supercritical fluid (SCF), adapting properties of both a gas and liquid.
- expands to fill its container (like a gas)
- has high density (like a liquid)
- Pros
- CO2 is a unique, highly selective "tunable solvent".
- can be "tuned" to selectivity extract different compound groups
- i.e. can separate (fractionate) terpenes from cannabinoids
- CO2 solvency properties can be "tuned" by adjusting its T and P.
- can function as a supercritical solvent (a SCF)
- can function as a subcritical solvent (a liquid)
- Supercritical fluid extraction (SFE):
- high pressure/high temperature (P= 1083 psi and T = 88℉)
- a strong solvent, which results in high yields
- can extract:
- all of the lighter molecular weights (volatile oils, light waxes)
- all of the heavier molecular weights (heavy waxes, lipids, fats, paraffin)
- good for separating out cannabinoids (as a group)
- Subcritical fluid extraction (SbFE):
- low pressure low temperature (P= 75 psi and T= 33 ℉)
- When supercritical CO2 T is dropped below 88℉, it changes phase (from a SCF to a liquid).
- a weaker solvent, which results in lower yields and longer extraction time
- extracts just the lower molecular weight compounds
- lower temperature prevents degradation of heat sensitive compounds
- good for separating out terpenes (as a group)
- Clean and safe solvent
- Non toxic
- Not flammable or explosive
- Environmentally friendly
- No need to purify
- No residual solvents remain in bulk extract
- kills microbial bacteria, mold, mildew and insect mites
- the only method that completely removes heavy metals and toxins
- runs without air, which prevents oxidation
- preserves more THCA and terpenes than other extraction methods
- Can be automated because CO2 is not explosive
- Low facility and operation cost
- Good for vape pens, terpenes and oils
- Cons
- High equipment cost due to high operating pressures
- Slow extraction times
- NOT good for live resin
- Hydrocarbon extraction: (butane, propane, hexane, naptha)
- Pros
- Low equipment cost due to low operating pressure
- High yields
- Medium extraction times
- Good for vape pens, distillates and dabbing products (shatter and live resin)
- Cons
- High facility and automation costs due to explosivity
- Residual toxic solvent remains in bulk extract
- NOT good for oils and infused products
- Ethanol extraction:
- Pros
- Low equipment cost due to atmospheric pressure
- High yields
- Fastest extraction times
- Good for vape pens, distillates and infused products
- Cons
- Moderate facility cost due to flammability (even though not explosive)
- High operation costs
- Ethanol is taxed
- Significant post processing energy to recover ethanol
- Residual solvents remain in bulk extract
- NOT good for dabbing and terpenes
Some secondary processing is required for each extraction method:
- Decarboxylation:
- converts the cannabinoid acids into cannabinoids
- a secondary process for most extraction methods
- a pre-extraction process when using CO2 method
- ground buds are placed in a forced air oven (not a vacuum oven)
- preheated to 240-250℉ (115.56-121.11℃)
- baked for 1-2 hours
- decreases extraction run time
- increases extraction yields
- Winterization:
- chemically separates the fats and waxes from the essential oils
- the bulk extract is mixed with 200 proof ethanol
- 10 : 1 ratio of ethanol : extract
- i.e. 800 mL ethanol : 80 grams extract
- mixture is placed in a sub-zero freezer (-84.6℉) (-64.78℃) for 24-48 hours
- Filtration:
- Winterized extract is poured through a vacuum filter
- physically separates the fats and waxes from the essential oils.
- Ethanol recovery:
- The filtered oil/ethanol suspension is put into a roto-vac
- flask is rotated in warm water (66.6℉) (19.22℃) to vaporize the ethanol
- vapors are sucked onto cold condensation coils, which distil (recover) the ethanol
- amber suspension is converted into a dark oil
- Vacuum oven - for dabs and shatters
- Distillation - for further concentration:
- actually a tertiary processing
- can result in pre distilled extracts with 80% THC, being further concentrated to as high as 90-95% THC
- not good for vape pens because all flavor is removed
The Human Endocannabinoid System
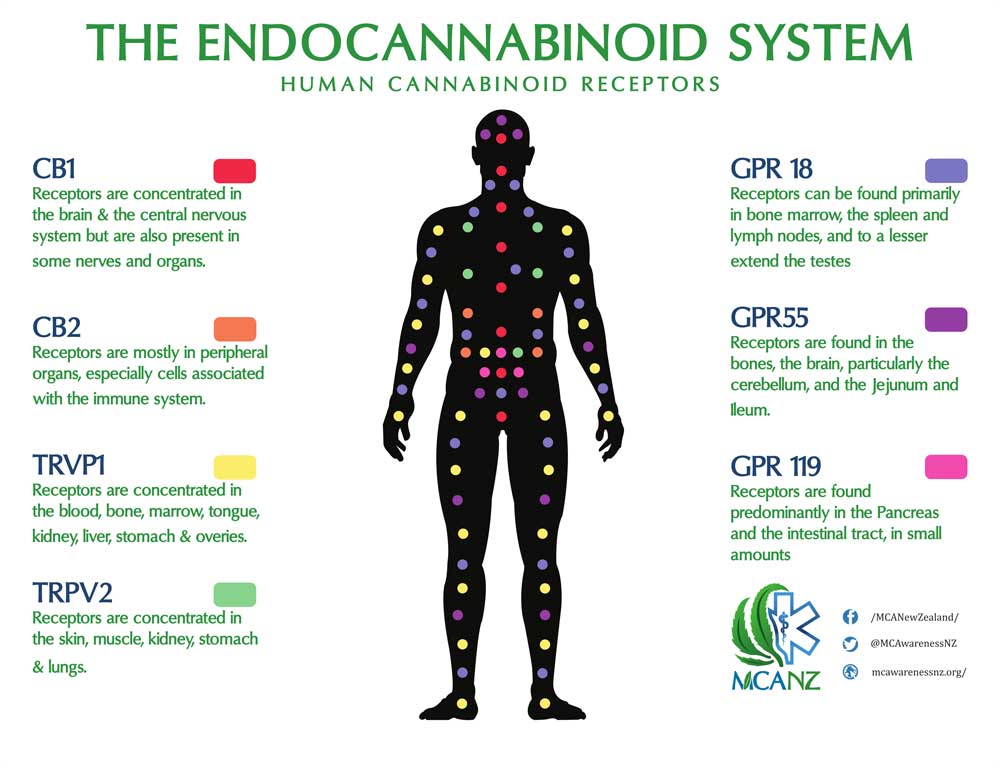
The Endocannabinoid System (ECS) is an endogenous (innate) system which . . .
- regulates physiological homeostasis through its interactions with:
- Cannabinoids
- endocannabinoids (made by the body)
- exocannabinoids (phytocannabinoids - from cannabis plants)
- cannabinoid receptors (targets of cannabinoids)
- regulatory enzymes
- Homeostasis is a dynamically-balanced state of internal variables:
- blood level of hormones, gases, ions and sugar
- blood pressure
- body temperature
- neurotransmission
- Maintaining these variables (within their homeostatic range) is vital to supporting optimal health.
- homeostasis affects: mood, pain, appetite, sleep, perception and cognitive functions.
- homeostasis can be disrupted by: illness, injury, toxins and medications.
- The ECS is present in humans and all animals (except insects).
- Cannabis modulates the ECS to facilitate homeostasis.
- Our bodies are designed to interact with cannabis.
The ECS was discovered in 1992, by Raphael Mechoulam (Hebrew University of Jerusalem), who observed that the ECS facilitates homeostasis through an elaborate, interactive, signaling scheme, involving cannabinoids, receptors and their regulatory enzymes.
There were several key research breakthroughs that led to this landmark discovery:
- In 1940 CBD was identified by Roger Adams
- In 1963 Mechoulam isolated and determined the molecular structure of CBD
- In 1964, Mechoulam identified and isolated THC for the first time.
- In 1988, Allyn Howlett and William Devane (Johns Hopkins University) discovered the first cannabinoid receptor in the brain of a rat.
- in 1990, Lisa Matsuda (National Institute of Mental Health) mapped the DNA sequence responsible for the expression of THC-sensitive receptors in a rat's brain.
- They were able to alter the genetics of rats, producing "knock out" rats that lacked CB1 receptors.
- By demonstrating that these "knock out" rats could did not get "high", they proved that "binding to CB1 receptors" is the mechanism by which THC works.
- in 1992, Mechoulam, Devane and Hanus, discovered the first endocannabinoid called Anandamide.
- In 1995, researchers (Mechoulam et.al) discovered that the two receptors (now deemed the CB1 and CB2 receptors) were found not only in rats, but within thousands of other species (including humans).
Due to the role cannabis played in discovering the ECS, it was aptly named "the endocannabinoid system".
The endocannabinoid system is VERY important because:
- Today's world is VERY inflammatory:
- Environmental Toxins:
- Herbicides
- Insecticides
- Heavy Metals
- Chronic Biological Infections:
- Bacteria
- Viruses
- Fungus
- Molds
- Inflammatory Diet / "Leaky gut"
- Endotoxins
- inflammation is VERY unhealthy:
- Immune Inflammation
- Autoimmune Disease
- Rheumatoid Arthritis
- Irritable Bowel Syndrome (IBS)
- Fibromyalgia/MS
- Skin / Psoriasis/ Eczema
- Chronic Infections
- Brain Inflammation
- Brain Fog / Migraine / Epilepsy
- Anxiety / PTSD
- ADD /ADHD /Autism
- Insomnia
Cannabiniods, though their interaction with the human endocannabinoid system,
support homeostasis and thus optimal health.
Cannabinoids can be classified by function or origin:
- Cannabinoids function in three basic ways:
- Agonists:
- bind to receptors
- Cannabinoid agonists stimulate G protein-coupled receptors (GPCRs) by binding to an "orthosteric" site on the receptor, which initiates a series of micro-conformational changes in the receptor structure, that ultimately leads to G-activation.
- Antagonists:
- block receptors
- Cannabinoid antagonists block activation of G proteins by binding to an "allosteric" site on the receptor that is involved in the G protein activation process, thereby precluding the ability of the orthosteric agonist-mediated conformational stimulus to execute activation.
- Modulators:
- do not bind or block receptors
- Unlike agonists and antagonists (whose action causes direct effects), These cannabinoids, modulate the environment "setting up" indirect effects
- Cannabinoids originate in three different ways:
- Endocannabinoids:
- "endogenous cannabinoids"- cannabis-like molecules (ligands), produced by the body.
- neural modulators (not neural transmitters)
- not stored in the body, so they are synthesized and released on demand.
- produced in post-synaptic neurons, then travel backwards to pre-synaptic neurons in the CB1 receptor (retrograde signaling) to inhibit neurotransmitter release, which influences other chemical reactions, producing a cascade effect.
- In the case of a head injury, or neuropathic pain, where there would normally be an abundance of glutamate, which could cause excitotoxicity (damage or death of neurons by excessive stimulation), this endoocannabinoidal mechanism can inhibit the excitotoxication.
- Two endocannabinoids have been discovered so far.
- Anandamide (aka Arachidonyl Ethanolamide or AEA):
- first endocannabinoid discovered (1992)
- a neural transmitter
- attaches to the same CB receptors as does THC.
- stimulates CB1 and CB2 receptors
- in parts of brain involved in reward, mood
- released during meditation and running
- named Anandamide (the "bliss" molecule)
- named after the word "Ananda" which means "supreme joy" (in Sanscrit)
- associated with "the runners high" effect
- anandamide not only targets the CB1 receptor, but also influences opioid and endorphin receptors.
- Contrary to what many believe, CBD does not turn into THC in the body, rather it simulates some THC effects, because it increases the relative gain of the ECS by upregulating anandamide.
- 2-arachidonoyl-glycerol (2-AG):
- second endocannabinoid discovered (1995)
- functions to "relax", eat, sleep, forget, protect
- endogenous agonist of the CB1 receptor and the primary endogenous ligand for the CB2 receptor
- predominantly found in the Central Nervous System
- released in mothers milk (along with anandamide, but in greater amount)
- can be neuro-endo-immune agonists
- Can also modulate:
- neurotransmission in the brain
- endocrine hormone production
- immune system response
- metabolized in the liver
- Exocannabinoids (Phytocannabinoids):
- formed when cannabinoid acids, such as THCA and CBDA, (naturally found in cannabis plants) are heated, resulting in CO2 being shed (decarboxylation) and neutral phytocannabinoids remaining.
- when taken into the body . . . they can be neurotransmitters or modulators.
- e.g., THC, CBD, CDN
- metabolized in the brain and the sites where they are being used
- Synthetic cannabinoids:
- synthesized in a lab
- e.g. ajulemic acid
- bind to cannabinoid receptors and causes affects
Cannabinoid receptors are a class of cell membrane receptors in the G protein-coupled receptor (GPCR) superfamily, which function as targets (the sites of activity) for cannabinoids in the ECS.
- contain seven transmembrane spanning domains.
- detect molecules outside the cell
- activate internal signal transduction pathways
- ultimately, cause cellular responses
- the largest class of receptors known
- widely dispersed throughout the body:
- Central Nervous System
- Cardio Vascular System
- Immune system
- Bone Marrow
- Intestines
- Bladder
- There are several types of endocannabinoid receptors:
- CB1 Receptors:
- Primarily found in the brain
- The most abundant G-protein-coupled receptor found in the brain
- highly expressed in:
- nociceptive areas of brain (responsible for sensation of pain)
- cerebellum and basal ganglia (regulates motor movements)
- limbic system (having to do with emotion)
- hippocampus (having to do with memory processing)
- reward pathways
- Although they are prominent in the substantia nigra and periaqueductal grey matter . . .
- they have very limited expression in the brainstem.
- not in medullary respiratory center . . .
- so unlike opioids (which have receptors in the medulla) an "over dose" of cannabis can not cause death by respiratory depression.
- expressed primarily on glutamatergic and GABAergic pre-synaptic interneurons, which when activated (depolarized) inhibit GABA-mediated neurotransmission, resulting in limited pre-synaptic calcium ions entry and thus less glutamate being released
- have major neuromodulatory functions, which are involved in:
- pain
- memory
- movement
- emotion
- appetite
- emesis
- seizure threshold
- GI motility/secretion
- Role characterized as "relax, eat, sleep, forget and protect"
- blocking CB1 receptors leads to depression
- There may be many other functions that we are not yet aware of.
- CB1 receptors have been found in the urinary tract and in parts of the reproductive system.
- Researchers believe they will find CB1 receptors in other parts of the body as well.
- CB2 Receptors:
- some expression in central and peripheral nervous system
- greatest expression is in the immune system
- circulating white blood cells
- macrophages
- B cells
- T cells
- the spleen, tonsils and thymus gland
- microglial cells (brain macrophages)
- hematopoietic cells (blood producing cells)
- in the skin (as is CB1)
- gastrointestinal system
- modulates intestinal inflammatory response
- shows great promise for Crohn's disease and IBS
- major immunomodulatory functions involved in pain and inflammation.
- regulates the release of cytokines
- assist in the communication between cells during immune responses
- encourages the appropriate cells to respond to inflammation and infection.
- limits fibrosis (build up of scar tissue)
- CB2 agonists have potential in treating hepatic fibrosis and related conditions
- Non Cannabinoid Receptors:
- TRP (Transient Receptor Potential):
- a superfamily of receptors, with a large number of cation channels
- modulate ion entry driving forces and Ca2+ and Mg2+ transport machinery in the plasma membrane, where most of them are located
- have important interactions with other proteins and often form signaling complexes
- Transient Receptor Potential Cation (TRPC) channels - include TRPV and TRPA receptors
- TRPV Receptors (Transient Receptor Potential Vanilloid Receptors):
- ionotropic receptors - form part of a ligand-gated ion channel, so that binding of ligand (e.g. a hormone or neurotransmitter) to the receptor causes opening of the channel, permitting ions to flow through it.
- present in skin
- associated with pain and itch on the skin
- CBD is a TRPV1 agonist
- which is why CBD is good for topical rashes and pain
- works as a sebostatic agent in acne
- While CB1 activation leads to a decrease in intracellular calcium and attenuation of synaptic transmission, anandamide binding to TRPV1 results in elevated calcium levels and potentiated synaptic transmission.
- TRPA Receptors (Transient Receptor Potential Ankyrin Receptors):
- Phytocannabinoids activate TRP channels of both TRPV1 and TRPA1 receptors.
- Serotonin Receptors (aka 5-hydroxytryptamine receptors or H-HT receptors):
- a group of G protein-coupled receptor and ligand-gated ion channels found in the central and peripheral nervous systems
- mediate both excitatory and inhibitory neurotransmission
- activated by the neurotransmitter serotonin, which acts as their natural ligand
- CBD is also an agonist of serotonin 1A receptors
- modulate the release of many neurotransmitters:
- glutamate
- GABA
- dopamine
- epinephrine / norepinephrine
- acetylcholine
- modulate the release of many hormones:
- oxytocin
- prolactin
- vasopressin
- cortisol
- corticotropin
- substance P
- influence various biological and neurological processes:
- aggression
- anxiety
- appetite
- cognition
- learning
- memory
- mood
- nausea
- sleep
- thermo-regulation
- the target of a variety of pharmaceutical and recreational drugs:
- many antidepressants
- antipsychotics
- anorectics
- antiemetics
- gastroprokinetic agents
- antimigraine agents
- hallucinogens
- entactogens
- GABA Receptors (Gamma-Amino Butyric Acid receptors):
- receptors that also control inflammation, pain, reward and anxiety
- Low GABA activity increases sensitivity to THC psychotomimetic effects
- Several terpenes can increase GABA activity
- Terpenes are anecdotally reported to reduce psychotomimetic effects
- Myrcene, alpha-pinene, phytol, and alpha-terpinolene could directly bind and increase activation of the GABA receptor.
- Phytol may also raise GABA levels by inhibiting its metabolism.
- Limonene raised GABA levels in rodents and its metabolites and could directly increase activation of the GABA receptor.
- Linalool could boost GABA activity in cells, even though it doesn't bind directly to the GABA receptor and could potentially have additional antipsychotic actions by inhibiting the NMDA receptor
- PPARs (Peroxisome Proliferator-Activated Receptors):
- a major class of nuclear hormone receptors
- function as transcription factors regulating the expression of genes
- Three types of PPARs have been identified: (α, δ and γ)
- Activation of all isoforms (primarily PPARα and γ), mediate some (but not all) of the analgesic, neuroprotective, neuronal function modulation, anti-inflammatory, metabolic, anti-tumor, gastrointestinal and cardiovascular effects of some cannabinoids.
- often in conjunction with activation of:
- CB1 and CB2 receptors
- the TRPV1 ion channel
- mediate some of the effects of endocannabinoid degradation/transport inhibition
- Researchers believe there are more (yet to be discovered) cannabinoid and non-cannabinoid receptors.
Regulatory Enzymes:
- required for making and breaking down endocannabinoids
- FAAH (fatty acid amide hydrolase) breaks down AEA
- MAGL (monoacylglycerol lipase) breaks down 2AG
Endocannabinoid tone is a term, which reflects the balance of the ECS components.
- the density of active cannabinoid receptors in the brain
- the levels of endocannabinoids and the rate at which they're made and broken down
- the amount of enzymes which make and break down the endocannbinoids
Endocannabinoid tone can be measured relatively, but technology does not exist to measure it absolutely.
- Serum levels of endocannabinoids in the blood may not reflect what is going on in the brain
- Direct measurements, such as spinal taps are too invasive to be practical.
- PET and MRI scans show promise in measuring absolute endocannabinoid tone, but currently can not.
CBD increases "endocannabinoid tone" -
- pools up endocannabinoids
- stimulates the production of 2AG
- achieves higher levels of AEA, by blocking the production of "fatty acid amide hydrolase" (FAAH), the enzyme which breaks down (hydrolyzes) AEA
- stabilizes neuroinflammation
- turns up glutiothione system and turns down the inflammatory processes
- stabilizes activated microglia
- stabilizes overactive glutamate receptors
Clinical Endocannabinoid Deficency (CED):
- a concept introduced by Dr. Ethan Russo in 2001, with subsequent publications in 2004 and 2016.
- According to Russo, If you don't have enough endocannabinoids:
- you may have pain, when you shouldn't.
- You may feel be nauseated, when you shouldn't.
- You may have a lowered seizure threshold.
- Russo theorized that a number of very common diseases seem to fit a pattern, that would be consistent with an endocannabinoid deficiency, specifically: migraine headaches, IBS and fibromyalgia.
- They're all hyperalgesic syndromes . . . the pain is way out of proportion to what it should be.
- The tissues look normal, yet there's something biochemically that's driving the pain.
- Additionally, they occur in the same individuals.
- If someone has a chronic problem with migraine there's a high likelihood they're going to have fibromyalgia at some point in their life; similarly, with the irritable bowel syndrome.
- In Italy, Sarchielli, et al, measured anandamide levels in cerebrospinal fluid.
- They did lumbar spinal taps on subjects with and without migraine headaches
- They found that subjects with migraine headaches had much lower levels than those who didn't.
- What are cannabinoids?
- What is hemp extract?
- Is CBD the same as hemp extract?
- What is hemp extract oil?
- Is hemp extract oil the same as hemp oil?
- Are hemp and marijuana the same thing?
- Will I get "high" if I use hemp extract oil?
- Is hemp extract oil addictive? Can someone overdose on hemp extract oil?
- Can someone fail a drug test if they use hemp extract oil?
- Is hemp extract oil legal?
- Do I need a prescription for hemp extract oil?
- Will hemp extract oil cure my condition?
- How much should I take? How do I administer the hemp extract oil?
- Can I use hemp extract oil when taking other medications?
- Do you ship your products interstate?
-
I've seen other hemp extract oil selling for MUCH less . . .
Why are Lipocana™ and Lipocanna™ so expensive?
FAQ
Q. What are cannabinoids?
A. Cannabinoids are a class of active compounds naturally occuring in the cannabis plant. THC and CBD are the most predominant and most extensively studied cannabinoids so far.
Q. What is hemp extract?
A. Hemp extract is a substance extracted from the aerial parts of the hemp plant. which contains non-intoxifying cannabinoids.
Q. Is CBD the same as hemp extract?
A. No. CBD or cannabidiol is one of many naturally occurring cannabinoids found in hemp extract. Isolated CBD is sold as a drug and is actually less effective in supporting health than a full spectrum extract oil, which benefits from the "the entourage effect". It is also worth noting that many unscrupulous marketers, make false CBD content label claims, where they equate the extract amount to CBD amount. This misrepresentation inflates the CBD content by a factor of two.
Q. What is hemp extract oil?
A. Hemp extract oil is an infusion of hemp extract into an oil
Q. Is hemp extract oil the same as hemp oil?
A. No. Hemp extract oil is extracted from the aerial parts of the hemp plant, whereas hemp oil, also know as hemp seed oil, is extracted from hemp seeds. Hemp extract oil is used as a health and wellness supplement and contains CBD (and VERY little THC). Hemp oil, on the other hand is used primarily in cooking and contains no CBD or THC.
Q. Are hemp and marijuana the same thing?
A. No. Both are from cannabis sativa or cannnabis indica species and both contain cannabinoids, however hemp is a low resin plant, while marijuana is a high resin plant. People often incorrectly think that hemp is high in CBD while marijuana is high in THC. This is not correct. Marijuana can be THC or CBD dominant, while hemp (being a low resin plant) is low in THC. That does not meant that hemp is high in CBD. It's actually not, which is why it takes a lot of hemp buds to produce a CBD rich extract. Hemp extract oil is produced/sold for health support, because federal law prohibits the transportation of marijuana extract products across state borders. Its kind of silly, considering that chemically there is no difference between marijuana and hemp extracts (of equal CBD/THC content). Go figure.
Q. Will I get "high" if I use hemp extract oil?
A. No. Hemp extract oil contains very little to no THC, which is the intoxifying compound in marijuana that causes the "high". Due to the low amounts of THC, hemp extract products will not cause you to feel "high".
Q. Is hemp extract oil addictive? Can someone overdose on hemp extract oil?
A. There is no current indication that hemp extract oil is addictive or can cause someone to overdose.
Q. Can someone fail a drug test if they use hemp extract oil?
A. While we cannot guarantee the results of any drug test, hemp extract oil, by nature, contains very low THC levels and should not show up in a standard drug test. Most work place drug tests measure for the intoxifying compound THC, not CBD.
Q. Is hemp extract legal?
A. Yes, it is legal under federal law. Our products are produced in a facility that is under a federally approved program, authorized under Section 7606 of the 2014 Farm Bill. Kentucky has established a program that allows for the production, manufacturing and shipping of hemp products across state lines. If you have any concern, we ask that you check the laws in the state where you reside.
Q. Do I need a prescription for hemp extract oil?
A. No, a prescription in not required to purchase hemp extract oil.
Q. Will hemp extract oil cure my condition?
A. Due to the FDA guidelines, we are prohibited from making any claims of health benefits associated with hemp extract oil, especially for specific medical conditions. To make the best decision on your health and wellness, we encourage everyone to do their own research and/or consult with their healthcare professional
Q. How much should I take? How do I administer the hemp extract oil?
A. The "right" amount will differ by person, as each of us are unique. Please check with your healthcare professional to determine the dosage that's best for you. Lipocana™ and Lipocanna™ are intended to be taken orally. Shake the bottle well before use. Place 1 full dropper under the tongue daily or as needed. Allow time for solution to absorb and swallow remaining oil. Please Note: One squeeze of the dropper will only fill the dropper half way. To get a full dropper, you will need to repeat.
Q. Can I use hemp extract oil when taking other medications?
A. Please check with your healthcare professional regarding using hemp extract oil with any medications you are taking.
Q. Do you ship your products interstate?
A. Yes. We ship across the USA.
Q. I've seen other hemp extract products selling for MUCH less . . .
Why are Lipocana™ and Lipocanna™ so expensive?
A.
- Most hemp product manufacturers are cheating you.
- They make false label claims:
-
Most of their products contain hemp oil (from seeds) . . .
NOT full spectrum hemp extract oil (from buds) as they claim. -
Of the few products that do contain full spectrum hemp extract oil . . .
most incorrectly equate the amount of hemp extract as the CBD amount,
(inflating the CBD amount by a factor of two). - Lipocana™ and Lipocanna™ make the correct label claims:
- and provides twice as much extract
- so you get what you pay for
How To Use
How much Lipocana™ or LIpocanna™ Hemp Extract Oil should I take every day?
The “right” amount of oil will differ by person, as each of us are unique. We do, however, have some general guidelines to help you out.
- Start small. Increase the amount, as needed, over a few days to get the desired effect.
- Split up the daily amount, taking half in the morning and the other half in the evening right before bed.
- Consult your healthcare professional regarding the use of hemp extract oil.
Which Lipocana™ or LIpocanna™ extract oil is the best for me?
- Each 2 oz. bottle contains approximately 59 full droppers of hemp extract oil.
-
One full dropper (1 mL) contains the following:
- Regular Strength (500 mg):
16.6 mg hemp extract oil with 8.33 mg Phytocannabinoid Diols - Extra Strength (1,500 mg):
50 mg hemp extract oil with 25 mg Phytocannabinoid Diols - Clnical Strength (6,000 mg):
200 mg hemp extract oil with 100 mg Phytocannabinoid Diols
- Regular Strength (500 mg):
How do I use Lipocanna?
- Loosen the top of the bottle, leaving the dropper in the bottle
- Squeeze and release the top of the dropper, which will fill the dropper half way.
- Place the dropper under your tongue and squeeze the top of the dropper to release the oil. Repeat this process until you've reached your desired amount.
- Hold the oil under your tongue allowing it to absorb for 1-2 minutes before swallowing.
FDA Disclaimer
This product is not for use by or sale to persons under the age of 18. This product should be used only as directed on the label. It should not be used if you are pregnant or nursing. Consult with a physician before use if you have a serious medical condition or use prescription medications. A doctor's advice should be sought before using this and any supplemental dietary product. All trademarks and copyrights are property of their respective owners and are not affiliated with nor do they endorse this product. These statements have not been evaluated by the FDA. This product is not intended to diagnose, treat, cure or prevent any disease. By using this site you agree to follow the Privacy Policy and all Terms & Conditions printed on this site. Void where prohibited by law.
Never Buy CBD Oil From Amazon
In July 2019, Wired reported that on more than one occasion, Amazon had been caught selling counterfeit supplements.
A related article in The Verge points out that
"Recent investigations find that bad actors are running amok on Amazon, and that the platform may be too big to police."
The investigation in question was performed by three Wall Street Journal reporters, who discovered 52 listings for supplements previously identified by the U.S. Food and Drug Administration and the U.S. Justice Department as containing illegally imported prescription drugs.
Adding insult to injury, dozens of these potentially dangerous items were also tagged "Amazon's Choice." As noted by The Verge, this label is based on customer ratings, price and average shipping time, but most consumers tend to interpret it as a seal of approval.
The Verge also points out another significant problem on Amazon's platform that results in customers being deceived: hijacked reviews. In some cases, the reviews you see under a product do not actually refer to the product currently for sale but for some previously listed product.
- These issues alone should be enough to disuade you from buying any supplements being sold on Amazon.
- But it gets even worse in the case of CBD . . .
On October 15, 2019 The Organic & Natural Health Association issued a warning that Amazon may be defrauding CBD consumers in two ways:
- by preventing genuine high-quality CBD products from being sold on their site . . .
- while simultaneously promoting and selling bogus products that claim to contain CBD, but don't.
- To investigate this paradox, The Organic & Natural Health Association hired a third-party laboratory to test Amazon's best-seller, New Age Premium Hemp Oil 1000 MG, for the presence of cannabinoids.
- The product tested positive for CBD:
- containing approximately 1% CBD (7.7 milligrams of CBD per 30 drops).
- even though the label does NOT claim to contain ANY CBD.
- Other products which DO make "CBD" label claims, were found to contain no CBD.
For the record, Amazon's policy prohibits the sale of CBD products, yet when you search for CBD in its search engine, you will get thousand of hits for products that match, because Amazon allows vendors to tag their products with whatever search words they want (including terms that are prohibited per its own policy).
According to Karen Howard, CEO and executive director of The Organic & Natural Health Association:
"Its really important for consumers to know that because Amazon doesn't allow the sale of products with CBD, there are no reputable companies selling CBD on their site.
Amazon states it has banned the sale of CBD supplements on its site, but allows advertising and tagging of CBD instead, inviting an influx of products to consumers that the FDA has been warning about.
Essentially, the public is being defrauded twice. First, Amazon's best-seller, New Age Premium Hemp Oil contains CBD even though its label does not list CBD. Second, those searching for CBD products are being misled into buying products containing zero CBD.
We will continue our analysis of these products on Amazon's site. Without any requirement for GMPs, consumers are running the risk of consuming products adulterated with processed oils, and we also know synthetic cannabinoid is in the market.
This deception Amazon is spoon-feeding consumers on CBD is highly irresponsible to millions of Americans in search of legitimate CBD supplements"
Lipocana™Full Spectrum Hemp Extract Oil - Regular Strength (500 mg)
- Regular Strength (500 mg)
- extracted:
- from certified organic buds
- with supercritical liquid CO2

- 1 bottle
- $42.95
- WARNING: Most hemp product manufacturers are cheating you.
- They make false label claims:
-
Most of their products contain hemp oil (from seeds) . . .
NOT full spectrum hemp extract oil (from buds) as they claim. -
Of the few products that do contain full spectrum hemp extract oil . . .
most incorrectly equate the amount of hemp extract as the CBD amount,
(inflating the CBD amount by a factor of two). - Lipocana™ makes the correct label claim:
- and provides twice as much extract
- so you get what you pay for
Lipocana Supplement Facts: REGULAR STRENGTH
|
Contains 2 fl oz (59.15 mL)
Serving Size: 1 mL (1 full dropper) (1/5 tsp) Servings per bottle: 60 |
||
| Per Servings | % Daily Value | |
|---|---|---|
Full Spectrum Hemp Extract Oil
|
16.6 mg | * |
Naturally contains 8.33 mg Phytocannabinoid Diols per serving.
Guaranteed to contain less than .3% THC
Other ingredients: MCT Coconut Oil
Directions: Take 1 full dropper (1 mL) daily, or as directed by your physician
Please Note: One squeeze of the dropper will only fill the dropper half way.
To get a full dropper, you will need to repeat.
Lipocana™Full Spectrum Hemp Extract Oil - Extra Strength (1,500 mg)
- Extra Strength (1,500 mg)
- extracted:
- from certified organic buds
- with supercritical liquid CO2

- 1 bottle
- $99.95
- WARNING: Most hemp product manufacturers are cheating you.
- They make false label claims:
-
Most of their products contain hemp oil (from seeds) . . .
NOT full spectrum hemp extract oil (from buds) as they claim. -
Of the few products that do contain full spectrum hemp extract oil . . .
most incorrectly equate the amount of hemp extract as the CBD amount,
(inflating the CBD amount by a factor of two). - Lipocana™ makes the correct label claim:
- and provides twice as much extract
- so you get what you pay for
Lipocana Supplement Facts: EXTRA STRENGTH
|
Contains 2 fl oz (59.15 mL)
Serving Size: 1 mL (1/5 tsp) Servings per bottle: 60 |
||
| Per Servings | % Daily Value | |
|---|---|---|
Full Spectrum Hemp Extract Oil
|
50 mg | * |
Naturally contains 25 mg Phytocannabinoid Diols per serving.
Guaranteed to contain less than .3% THC
Other ingredients: MCT Coconut Oil
Directions: Take 1 full dropper (1 mL) daily, or as directed by your physician
Please Note: One squeeze of the dropper will only fill the dropper half way.
To get a full dropper, you will need to repeat.
Lipocanna™Full Spectrum Hemp Extract Oil - Clinical Strength (6,000 mg)
- Clinical Strength (6,000 mg)
- extracted:
- from certified organic buds
- with supercritical liquid CO2

- 1 bottle
- $219.95
- WARNING: Most hemp product manufacturers are cheating you.
- They make false label claims:
-
Most of their products contain hemp oil (from seeds) . . .
NOT full spectrum hemp extract oil (from buds) as they claim. -
Of the few products that do contain full spectrum hemp extract oil . . .
most incorrectly equate the amount of hemp extract as the CBD amount,
(inflating the CBD amount by a factor of two). - Lipocanna™ makes the correct label claim:
- and provides twice as much extract
- so you get what you pay for
Lipocana Supplement Facts: CLINICAL STRENGTH
|
Contains 2 fl oz (59.15 mL)
Serving Size: 1 mL (1/5 tsp) Servings per bottle: 60 |
||
| Per Servings | % Daily Value | |
|---|---|---|
Full Spectrum Hemp Extract Oil
|
200 mg | * |
Naturally contains 100 mg Phytocannabinoid Diols per serving.
Guaranteed to contain less than .3% THC
Other ingredients: MCT Coconut Oil
Directions: Take 1 full dropper (1 mL) daily, or as directed by your physician
Please Note: One squeeze of the dropper will only fill the dropper half way.
To get a full dropper, you will need to repeat.
Other Products Available from: NHS Global Distributors, Inc.



Prostate Miracle®
Trusted by thousands to support healthy urinary flow and prostate health.
read more
Estrogen Balance®
A natural formula for Men & Women, combining: D.I.M., Quercetin and Flaxseed.
read more

Sea of Greens™
A Whole-Superfood supplement, combining an optimal blend of sea vegetables and Freshwater algae.
read more
Pectin Plus®
Supports healthy detoxification, healthy blood pressure, healthy cholesterol levels and prostate health
read more
Immune System Plus™
An immune system support formula based on Beta Glutan, which is unsurpassed in it's ability to help support a healthy immune response.
read more
Contact
P.O. Box 271
Camarillo, CA 93011-0271
International: 1.805.322.0005

Thank you for visiting Lipocanna.com
This information here within is designed to provide accurate information in regard to the subject matter covered. It is provided with the understanding that NHS Global Distributors, Inc. is not engaged in rendering medical advice. If expert assistance is required, the services of a competent medical professional should be sought. These statements have not been evaluated by the Food and Drug Administration. These products are not intended to diagnose, treat, cure or prevent any disease. Always read and follow manufacturer's directions that come with this product.
You are protected by the FDA Dietary Supplement and Nonprescription Drug Consumer Protection Act
please call 877.965.2140 or Click here to report any Adverse Reaction with LipoCanna™.